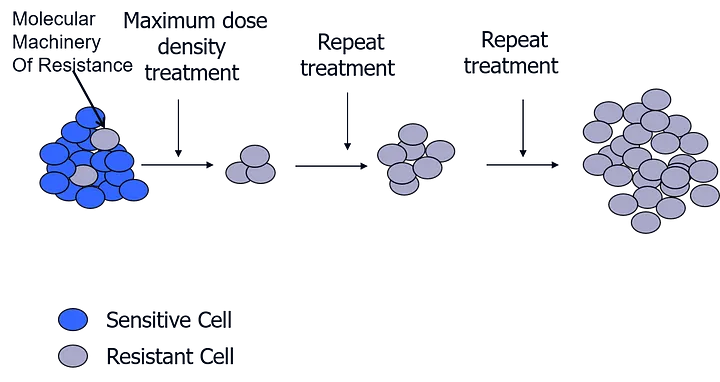
Dr. Gatenby’s team’s method is based on the understanding that any tumor comprises a mixed population of cancerous cells. All these cells want to do is to keep multiplying. As the tumor environment has limited resources, these multiple cells compete with each other. Cancer cells also develop the ability to change and adapt to their environment to keep multiplying. So, if a tumor is subjected to a treatment, some of the cells in the mixed population are selected because they are resistant to treatment. However, this can come at a cost.
Adaptive therapy leverages the cost of developing resistance. Since the sensitive cells do not have the burden of the resistance mechanisms that the resistant cells have, the sensitive cells have an advantage. When treatment is paused, sensitive cells outcompete the resistant cells. The strategy is to use the sensitive cells that you can control, to control the resistant cells that you cannot control. In other words, you change the dynamics within a tumor to improve the outcomes of treatment.
Here are several key underlying principles of a treatment strategy that can control the evolution of an advanced cancer:
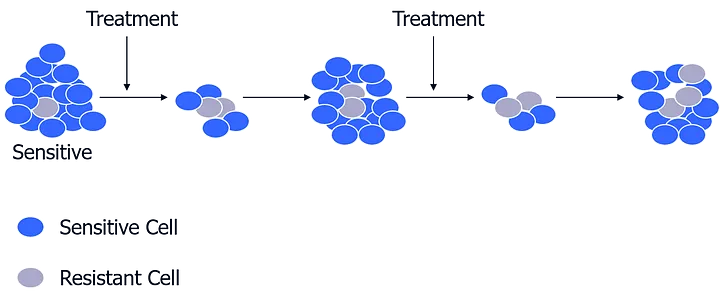
- Apply a low dose: Hit the tumours with enough treatment to perturb their system, but not so much to kill all the sensitive cells, thereby leaving the environment free for the resistant cells to proliferate. The resistant cells can be controlled by keeping enough of the sensitive cells around.
- Apply treatment combinations (first strike, second strike): Lacking magic bullets, metastatic cancers can be kept under control through a strategic combination of pretty good bullets. None of these bullets could by themselves cure the cancer, but the combination could.
- Sequence treatments (not a combination cocktail): If you have a combination cocktail, especially as a first strike, you’re applying the therapy to the largest possible population. The heterogeneity of the cancer cells is such that almost certainly, you will find tumor cells that will be resistant to the combination. It is better to hit the cancer with therapies in sequence, as each knocks the population down and can drive it to extinction.
- Use mathematical models as a guide: Having a hypothesis and a simulation of what should happen based on evolutionary theory helps in understanding why and enables insights from much smaller trial cohorts.